
This case is a very good example of an unstable and highly aggressive double major scoliosis that responded to therapy over a 2-week intensive period of care; convex to the left in the lumbar spine and to the right in the thoracic spine. The curves are evenly spaced across the midline – i.e. the centre of gravity. Click here to jump to results
Background
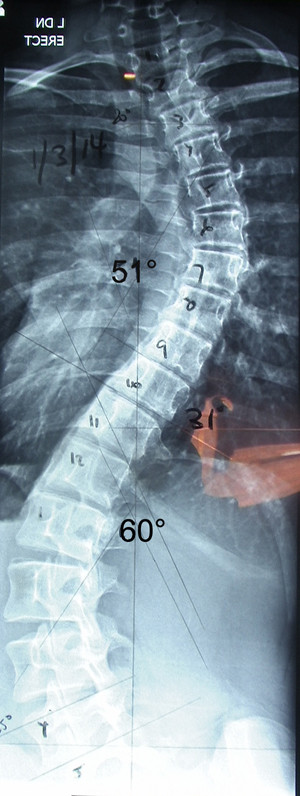
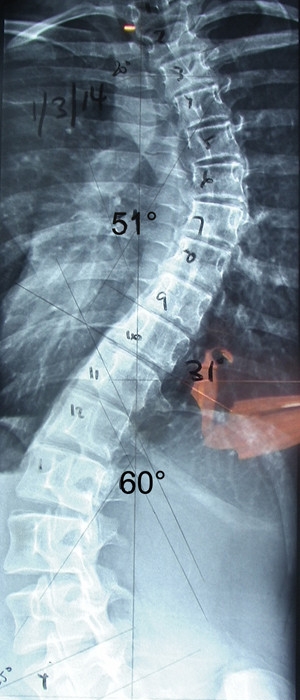
This thinly built 14 year-old high school student presented with 2 rapidly aggressive curves now measuring 51˚ – 55˚ and 60˚, a doubling in just two years. She experienced little discomfort. Her appearance indicated some leaning to the left though the symmetrical nature of the curve (similar angles) disguised the scoliosis. As the overall appearance did not indicate the degree or severity of such curves, the discovery of the scoliosis naturally came as a shock to both the young lady and her parents. The mother made the discovery upon noticing bumps upon her daughter’s forward bending. With marked progression the family were keen to prevent surgery.
Treatment
Scoliosis care commenced with a 2-week daily intensive programme.
Specific exercises were introduced in order to find the most effective way forward.
Care began with a series of reduction exercises that were maintained throughout the intensive period. Our client was able to attend school throughout the intensive programme.
Results
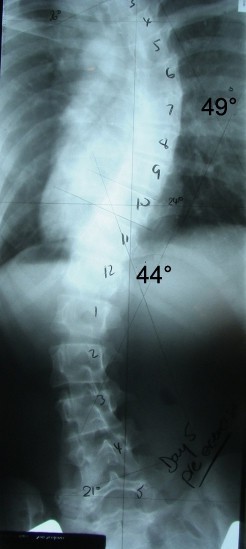
The x-ray images indicate a decrease in the upper curve from 51 to 49 degrees and a large decrease in the lower curve from 60 to 44 degrees (16 degrees over the 2-week intensive). The vertebral angles were recorded as follows:
| Tilt of vertebrae (Vert.) from Horizontal – (measured in degrees) | |||
| Day 0 | Day 5 | Day 12 | |
| Apical Vert. (T5) | 20 | 20 | 20 |
| Pivot Vert. (T11) | 32 | 24 | 24 |
| Terminal Vert. (L4) | 26 | 21 | 21 |
| Top Cobb Angle | 51 | 49 | 49 |
| Bottom Cobb Angle | 60 | 44 | 44 |
Discussion
This client demonstrates an encouraging initial response over a 2-week period. Early signs of curve reduction and muscle memory were demonstrated.
A pre-exercise x-ray (Day 12) was taken to see if early results were maintained through the development of muscle memory. A more centered and symmetrical structure was seen at the end of 2 weeks. This is a positive start to achieving stabilization and possible reduction in the long term.
Swift changes of this magnitude defy current medical opinion and are suggestive of a highly unstable curve. For curves of this size and rate of progression, only one option is generally presented – Surgery. Whilst the natural history of this type of curve is of rapid progression, corrective forces (specific exercises) and the modification and / or elimination of harmful behaviors, caused not only a reduction but a possible stabilization strategy. Surgery is less of a chance going forward.
A behavioral / exercise model (finesse) is highly recommended instead of a surgical approach (force) for large and aggressive curves with far less physical and psychological risk from the therapy itself.There is hope for improvement in many large curves regardless of age. (see previous cases)
Whilst the cause of scoliosis is rarely identified, it is highly recommended that the pursuit of such driving factors be closely investigated. A logical and systematic analysis of behaviours may uncover dangerous factors that cause progression. Long-term success is dependent on uncovering causes to scoliosis. An effective strategy that reduces risk factors with the addition and implementation of specific spinal isometric exercises lead to the initial reduction above.
At all times curvature control is best done early so as to prevent progression and further deformity. Delay only leads to a poorer quality of life, more concern, a feeling of being out of control and also increased financial pressures.
With aggressive curves monitoring over a well identified and dangerous period (growth spurt during adolescence) can be highly advantageous. This not only minimises progression but assists with reduction. As the spine grows – it has the potential to grow taller not just sideways. Taking action rather than following dangerous ‘Watch and Wait’ advice is advised.
The associated risks with surgery and bracing are considerable and can be avoided with a behavioural / risk analysis and spinal isometric approach.
As stated above, the forward bending test to detect scoliosis can be too late for the early management of scoliosis. For a more sensitive and accurate examination please call or send an email to [email protected].
All results on this site have been achieved without bracing, machines, surgery or medications.
These results are not indicative that this can be achieved in every case.
See Also:
- Scoliosis Case Study 1
- Scoliosis Case Study 2
- Scoliosis Case Study 3
- Scoliosis Case Study 5
- Scoliosis Case Study 6 (NEW)